

CBT vs DBT
If you’ve been looking into therapy options for depression, anxiety, borderline
personality disorder, or trauma, you’ve likely come across two names: Cognitive
Behavioral Therapy (CBT) and Dialectical Behavior Therapy (DBT). Both are evidence
based, both are widely used, and both are often confused with each other.
At Zen Minds Psychiatry in Boston, we believe that choosing the right therapy starts
with understanding what each one is actually designed to do — and matching it to your
specific needs. This guide covers everything you need to know about CBT vs DBT
therapy: the origins, the methods, the types of sessions, what conditions each treats
best, and how to make the right choice.
What Is CBT (Cognitive Behavioral Therapy)?
Cognitive Behavioral Therapy, or CBT, is one of the most extensively researched
psychotherapies in the world. Developed in the 1960s by psychiatrist Aaron Beck, CBT
is built on a deceptively simple premise: our thoughts, feelings, and behaviors are
interconnected. When we change how we think, we change how we feel and act. You
can read more about Cognitive Behavioral Therapy at Zen Minds Psychiatry and how
Dr. Chopra integrates it into comprehensive psychiatric care.
Core Principles of CBT:
• Cognitive restructuring: Identifying and challenging distorted or unhelpful thought
patterns (cognitive distortions), such as catastrophizing, all-or-nothing thinking, or
mind reading.
• Behavioral activation: Gradually re-engaging with activities to break cycles of
avoidance and low mood.
• Present-focused: CBT addresses current problems rather than exploring the
deep roots of the past.
• Skill-based and time-limited: Most CBT programs run for 12–20 sessions with
clear goals.
• Collaborative: Therapist and patient work together to identify patterns and
practice new responses.
What Does CBT Treat?
CBT has the strongest evidence base of any psychotherapy and is effective for a wide
range of conditions:
• Major Depressive Disorder (MDD)
• Generalized Anxiety Disorder (GAD)
• Panic Disorder and Social Anxiety
• Obsessive-Compulsive Disorder (OCD)
• PTSD (particularly trauma-focused CBT)
• ADHD (executive function and behavioral skills)
• Insomnia (CBT-I is the first-line treatment for chronic insomnia)
• Eating Disorders
• Adjustment Disorder with Anxiety
For patients dealing with depression, a tailored CBT approach is often part of our
integrated treatment plan alongside medication management. See our page on major
depressive disorder treatment in Boston for more detail.
What Is DBT (Dialectical Behavior Therapy)?
Dialectical Behavior Therapy was developed in the late 1980s by psychologist Marsha
Linehan, originally to treat individuals with borderline personality disorder (BPD) who
were chronically suicidal. The word ‘dialectical’ refers to the core tension at the heart of
the therapy: the balance between acceptance and change.
DBT builds on CBT’s cognitive and behavioral techniques but adds three critical
components that make it uniquely suited to individuals who experience intense, rapidly
shifting emotions: mindfulness, distress tolerance, and interpersonal effectiveness.
“DBT teaches people that they can change their lives even if they aren’t
responsible for all of their problems.” — Marsha Linehan, PhD (paraphrased from
her foundational work on DBT).
The Four Skill Modules of DBT
• Mindfulness: The foundation of DBT. Patients learn to observe and describe
their experiences without judgment — developing awareness of what is
happening in the present moment without being swept away by it.
• Distress Tolerance: Skills for surviving crisis moments without making them
worse. Techniques include TIPP (Temperature, Intense exercise, Paced
breathing, Progressive relaxation) and radical acceptance — fully acknowledging
reality without fighting it.
• Emotion Regulation: Understanding and naming emotions, identifying factors
that increase vulnerability, and building positive experiences to create emotional
resilience.
• Interpersonal Effectiveness: Navigating relationships skillfully — how to ask for
what you need, set boundaries, and maintain self-respect while preserving
important relationships.
What Does DBT Treat?
• Borderline Personality Disorder (BPD) — DBT is the gold-standard, most
evidence-backed treatment
• Chronic suicidal ideation and self-harm behaviors
• PTSD — particularly complex or relational trauma
• Substance use disorders
• Eating disorders, particularly bulimia nervosa and binge eating
• Depression that hasn’t responded adequately to other approaches
• Adolescents with emotional dysregulation
If you’re trying to understand whether BPD or another mood disorder is the right
diagnosis, our companion blog Borderline Personality Disorder vs Bipolar Disorder
walks through the key distinctions in detail.
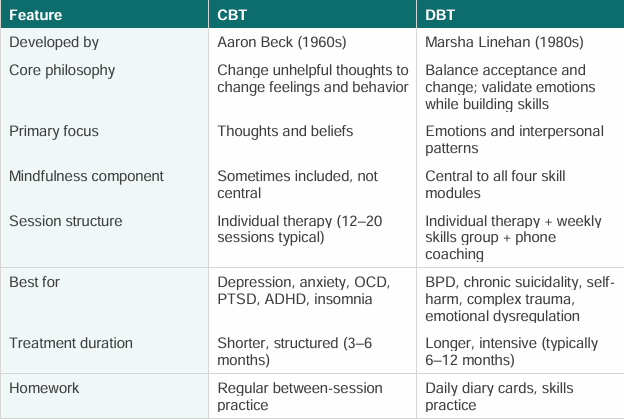
CBT vs DBT Therapy: Key Differences
Types of Sessions: What to Expect in CBT vs DBT
CBT Sessions:
A typical CBT session is structured and goal-oriented. You and your therapist will:
• Review your mood and any significant events since the last session
• Examine specific thoughts that contributed to distress (using thought records)
• Challenge cognitive distortions through Socratic questioning
• Practice alternative, more balanced thinking patterns
• Assign and review between-session homework (thought journals, behavioral
experiments)
Sessions are usually 50–60 minutes, held weekly. Because CBT is relatively time
limited, patients typically notice measurable improvement within the first 6–8 sessions.
DBT Sessions:
Full-model DBT is more intensive than standard CBT and involves three components:
• Individual therapy (weekly, 50–60 minutes): Focused on applying DBT skills to
real problems the patient is facing. The therapist works through a hierarchy: life
threatening behaviors first, then therapy-interfering behaviors, then quality-of-life
issues.
• Skills training group (weekly, 90–120 minutes): Led by a DBT therapist, this is
a psychoeducational group — not a traditional support group. Patients learn and
practice the four skill modules in a structured curriculum that cycles over
approximately 24 weeks.
• Phone coaching: Between sessions, patients can contact their individual
therapist for brief calls to get help applying skills in crisis moments. This is a
unique feature of DBT not found in standard CBT.
Simplified DBT (individual skills training without a group component) is also
available and may be appropriate depending on the patient’s presentation and
goals. This is something Dr. Chopra can help you evaluate.
CBT vs DBT: Which Therapy Is Right for You?
The honest answer is that the right therapy depends on your specific diagnosis, the
nature of your emotional patterns, and what you’re trying to change. Here are some
general clinical guidelines:
CBT may be the better fit if you:
• Are dealing with depression, generalized anxiety, panic disorder, social anxiety,
or OCD
• Want a structured, time-limited approach with clear goals
• Struggle primarily with negative thought patterns that you recognize intellectually
but can’t seem to shake
• Have insomnia that isn’t responding to medication alone (CBT-I is first-line
treatment)
• Are managing ADHD and need help with executive function, time management,
and impulsivity.
DBT may be the better fit if you:
• Have been diagnosed with borderline personality disorder or suspect you might
have it
• Struggle with intense, rapidly shifting emotions that are difficult to regulate
• Have a history of self-harm, chronic suicidal thoughts, or repeated crisis episodes
• Find that understanding your negative thoughts isn’t enough — you need more
radical emotional skills
• Have complex or relational trauma where emotional dysregulation is central
• Are dealing with eating disorder behaviors or substance use alongside emotional
instability.
When both may be used:
It’s worth noting that DBT was developed from CBT — it shares the same cognitive
behavioral foundation. Many clinicians integrate techniques from both depending on
what a patient needs. In complex presentations, such as bipolar disorder co-occurring
with BPD, a tailored treatment approach drawing on both frameworks may be most
effective.
What About Medication? Do You Still Need It?
Therapy and medication are not an either/or choice — for most psychiatric conditions,
the evidence supports combining both. CBT and DBT work best when underlying
biological contributors to mood, anxiety, or dysregulation are also addressed.
At Zen Minds Psychiatry, Dr. Chopra provides integrated psychiatric care that combines
medication management with a deep understanding of therapy frameworks. Whether
you’re managing bipolar disorder, depression, anxiety, or a personality disorder, your
treatment plan will be built around what the evidence says works — not a one-size-fits
all protocol.
Frequently Asked Questions About CBT vs DBT
Is DBT harder than CBT?
DBT is more intensive than standard CBT — particularly full-model DBT, which involves
individual therapy, a weekly skills group, and phone coaching. This intensity is
intentional. The patients DBT was designed for have complex needs that require more
sustained support. That said, simplified or adapted DBT approaches exist and may be
appropriate depending on your situation.
Can I do CBT and DBT at the same time?
In most cases, no — mixing two distinct therapy frameworks simultaneously can dilute
the effectiveness of both. However, a skilled clinician will draw on relevant techniques
from each as appropriate to your presentation. This is different from formally undergoing
both as separate treatment protocols.
How long does CBT take to work?
Most people notice meaningful symptom improvement within 6–12 sessions of CBT.
Full treatment courses typically run 12–20 sessions over 3–5 months. For conditions
like OCD, longer treatment may be needed.
How long does DBT take?
Standard DBT spans approximately 12 months, cycling through the four skill modules
twice. Research suggests that sustained engagement over this period produces the
most durable outcomes, particularly for BPD and chronic suicidality.
Is CBT covered by insurance?
Yes — CBT and DBT are recognized, evidence-based treatments and are typically
covered by major insurance plans. At Zen Minds Psychiatry, we accept most major
insurance plans and offer out-of-network options as well.
Can DBT help with bipolar disorder?
DBT was not originally designed for bipolar disorder, but adaptations of DBT have
shown promise in helping patients with bipolar disorder manage emotional reactivity and
improve interpersonal functioning. For bipolar disorder, however, mood stabilizing
medication remains the primary treatment.
What is the difference between CBT and talk therapy?
‘Talk therapy’ is a general term that encompasses all forms of psychotherapy. CBT and
DBT are specific, structured forms of talk therapy grounded in empirical research and
delivered according to established protocols. Unstructured supportive counseling, while
valuable, is different from these evidence-based approaches.
Getting Started in Boston
Whether you’re trying to find the right therapy for yourself or a loved one, the first step is
an accurate psychiatric assessment. At Zen Minds Psychiatry, Dr. Amit Chopra offers
comprehensive evaluations that consider your diagnosis, history, and goals before
recommending a treatment path. We work with you — not just a checklist.
We treat conditions including depression, anxiety, OCD, PTSD, ADHD, and bipolar
disorder. Our psychiatric services page outlines the full range of what we offer. We
accept new patients for both in-person visits in Boston and telepsychiatry across
Massachusetts. Ready to find out which therapy is right for you? Book a consultation with Dr.
Chopra at Zen Minds Psychiatry — call (626) 594-6042 or book online. We offer
in-person and virtual visits across Massachusetts.
Book your appointment at Zen Minds Psychiatry today and take the first step toward
care that actually fits.