

Major Depressive Disorder ICD-10
If you’ve been given a diagnosis of major depressive disorder and seen the letters and numbers “F33.1” or “F32.9” on your paperwork, you’re not alone in wondering what they mean. These are ICD-10 codes — the universal system that clinicians, hospitals, and insurance companies use to classify and communicate diagnoses. Understanding your code is not just administrative detail. It tells you something specific about how your depression has been categorized, how severe it is considered to be, and whether it has occurred before.
This guide explains the ICD-10 coding system for major depressive disorder clearly and completely — from the basic structure of the F32 and F33 categories, to what F33.1 specifically means, to how these codes shape treatment decisions. If you’re seeking expert care for depression in Boston, Zen Minds Psychiatry provides comprehensive, evidence-based treatment led by Dr. Amit Chopra, MD — Harvard Medical School faculty, MGH-affiliated, and Mayo Clinic-trained with over 20 years of experience in complex mood disorders.
What Is the ICD-10 Code for Major Depressive Disorder?
ICD-10 stands for the International Classification of Diseases, 10th Revision. In the United States, clinicians use a clinical modification called ICD-10-CM to diagnose and document mental health conditions for both clinical records and insurance billing. Major depressive disorder (MDD) falls under the broad category of Mood (Affective) Disorders, classified between F30 and F39.
There is no single ICD-10 code for major depressive disorder. Instead, MDD is coded across a family of specific codes organized by two key variables: whether the depression is a first (single) episode or a recurrent pattern, and how severe the current episode is.
The two primary categories are:
- F32 — Major Depressive Disorder, Single Episode: Used when the patient is experiencing their first documented lifetime episode of major depression, with no prior episodes on record.
- F33 — Major Depressive Disorder, Recurrent: Used when the patient has experienced at least two distinct major depressive episodes separated by at least two months of relative remission.
Key principle: The choice between F32 and F33 is not about severity — it is about history. A patient in their third depressive episode with mild symptoms is coded F33.0, not F32.0. Getting this right matters for insurance reimbursement, treatment authorization, and longitudinal clinical tracking.
The Full ICD-10 Code Table for Major Depressive Disorder
Here is a complete reference of the F32 and F33 codes used for major depressive disorder:
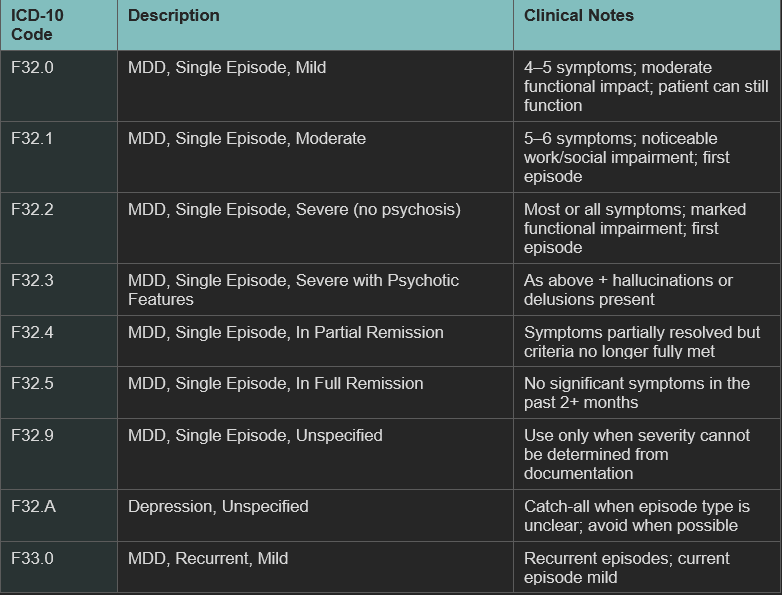
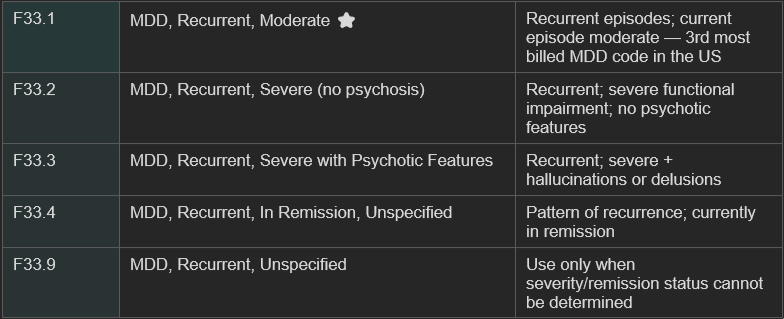
ICD-10 Code Table for Major Depressive Disorder
F33.1 is the ICD-10 code for Major Depressive Disorder, Recurrent, Moderate. It is one of the most commonly assigned MDD codes in clinical practice — and the third most frequently billed ICD-10 code across mental health practices in the United States.
Breaking it down:
- F33 — Recurrent: The patient has experienced at least two distinct major depressive episodes in their lifetime, separated by at least two months during which they did not meet full criteria for MDD.
- .1 — Moderate: The current episode meets criteria for moderate severity, meaning symptoms are significant enough to cause noticeable impairment in daily functioning — at work, in relationships, or in self-care — but the person has not lost the ability to function entirely.
What Does Moderate Severity Mean in Practice?
Moderate depression sits between mild and severe on the clinical spectrum. A patient with F33.1 typically presents with:
- Five or more DSM-5 symptoms of major depression present for two or more weeks
- Either depressed mood or loss of interest/pleasure (anhedonia) must be one of the five
- Symptoms causing meaningful disruption to work performance, social relationships, or daily routines
- Functional impairment that others may notice — reduced output at work, withdrawal from relationships, neglect of responsibilities
- Not so severe that the person is completely unable to function or requires hospitalization
The nine DSM-5 symptoms assessed for this diagnosis are: depressed mood, loss of interest or pleasure (anhedonia), significant weight change or appetite disturbance, sleep disturbance (insomnia or hypersomnia), psychomotor agitation or retardation observable by others, fatigue or loss of energy, feelings of worthlessness or excessive guilt, difficulty concentrating or making decisions, and recurrent thoughts of death or suicidal ideation.
F33.1 means you’ve been here before. The recurrence designation matters clinically: a second or third episode of depression carries a higher risk of future episodes than a first. This shapes both the intensity of treatment and the timeline of maintenance therapy.
F33.1 vs. Similar Codes: How Clinicians Choose
Several codes are easily confused with F33.1. Here is how they differ:
- 1 vs F33.1: Both describe moderate depression. The difference is recurrence. F32.1 is a first lifetime episode; F33.1 is a second or later episode. History matters.
- 0 vs F33.1: Both describe recurrent MDD. The difference is severity. F33.0 is mild recurrent depression; F33.1 is moderate. Severity is determined by symptom count and functional impact.
- 2 vs F33.1: Both describe recurrent MDD. F33.2 is severe — the patient’s ability to function is substantially lost. F33.1 is the step below that: impaired, but not collapsed.
- 9 vs F33.1: F33.9 is a vague fallback code. F33.1 requires documented severity — five or more symptoms, functional impairment, recurrent history. Clinicians should use F33.1 only when the documentation supports it.
DSM-5 Specifiers That May Accompany F33.1
In clinical documentation, F33.1 is often paired with DSM-5 specifiers that provide additional clinical precision:
- With anxious distress: Anxiety symptoms are prominent alongside depression — common in clinical practice and affects treatment choice.
- With seasonal pattern: Episodes reliably onset and remit at the same time each year (commonly fall/winter).
- With peripartum onset: Episodes begin during pregnancy or within four weeks postpartum.
- With melancholic features: Characterized by profound anhedonia, early morning awakening, and marked psychomotor changes.
- With atypical features: Mood brightens in response to positive events; hypersomnia and increased appetite rather than insomnia and weight loss.
These specifiers do not change the ICD-10 code itself, but they do shape treatment decisions significantly. A clinician who documents F33.1 with melancholic features will approach medication management differently than one documenting F33.1 with atypical features.
Why ICD-10 Codes Matter for Patients — Not Just Billing
Many patients assume ICD-10 codes are purely administrative — something that exists for insurance purposes and has nothing to do with their actual care. That is not accurate.
Your code affects your treatment authorization
Insurance companies use ICD-10 codes to determine what treatments they will cover, for how long, and at what level of intensity. A patient coded F33.1 may have more straightforward access to ongoing therapy and medication management than one coded F32.9, because the recurrent and moderate specification provides clinical justification for more comprehensive care.
Your code shapes your treatment plan
A first episode of mild depression (F32.0) is treated differently from recurrent moderate depression (F33.1). Recurrence is a powerful predictor of future episodes — research suggests that after a second episode, the probability of a third exceeds 70%. This changes the calculus around maintenance antidepressant therapy, the duration of treatment, and the role of therapy in relapse prevention.
Your code reflects the clinician’s clinical reasoning
The code your psychiatrist assigns represents a judgment — about the nature, severity, and history of your depression. If you’re uncertain what your code means or why it was assigned, it is entirely appropriate to ask your clinician for an explanation. Understanding your diagnosis is part of informed care.
How Is MDD Diagnosed and Coded in Clinical Practice?
At Zen Minds Psychiatry, the diagnostic process for major depressive disorder begins with a comprehensive psychiatric evaluation — typically 60 to 90 minutes for an initial visit. Dr. Chopra reviews:
- Full mood history: the timeline of all depressive episodes, their duration, severity, and triggers
- Sleep patterns: both because poor sleep worsens depression and because sleep disorders (insomnia, sleep apnea, circadian rhythm disturbance) can directly cause or mimic depressive symptoms
- Prior treatment history: medications tried, doses, duration, and response
- Family psychiatric history
- Validated rating scales such as the PHQ-9, which provides a standardized measure of symptom severity across the nine DSM-5 criteria
- Ruling out conditions that can mimic MDD: hypothyroidism, vitamin D deficiency, anemia, undiagnosed bipolar disorder, and substance use.
Dr. Chopra’s dual board certification in psychiatry and sleep medicine means that sleep disorders — which are both a cause and a consequence of depression — are evaluated as part of every assessment. This integrated approach is not available at most Boston psychiatry practices.
Major Depressive Disorder Treatment: What Follows the Diagnosis?
Once a diagnosis — and the appropriate ICD-10 code — has been assigned, treatment begins. At Zen Minds Psychiatry, major depressive disorder treatment in Boston is individualized based on episode history, severity, comorbidities, and prior treatment response. There is no protocol applied to a code — there is a protocol designed around you.
Medication Management
For F33.1 (recurrent, moderate depression), medication is almost always part of the treatment plan. First-line antidepressants include SSRIs and SNRIs, selected based on your symptom profile, history of response, side effect tolerance, and any co-occurring conditions. For recurrent depression, maintenance therapy — continuing medication beyond symptom resolution — is a key part of preventing relapse.
Psychotherapy
Cognitive Behavioral Therapy (CBT) is the most evidence-based psychotherapy for major depressive disorder, with strong data showing it reduces relapse risk when continued after acute symptom improvement. Learn more about how CBT works in depression treatment in our detailed guide.
Integrated Sleep and Mood Care
Disrupted sleep is both a symptom and a driver of depression. Dr. Chopra’s background in sleep medicine means that CBT for Insomnia (CBT-I), circadian rhythm work, and sleep disorder diagnosis are integrated into depression care — not treated as separate concerns.
When Standard Treatments Haven’t Worked
For patients with F33.x codes who have not responded adequately to first or second-line treatments, Zen Minds Psychiatry specializes in treatment-resistant presentations. This includes evaluation for alternative diagnoses such as bipolar disorder (which can be masked as recurrent MDD), augmentation strategies, and advanced treatment options. See our guide on borderline personality disorder vs bipolar disorder to understand how misdiagnosis can affect treatment outcomes.
Frequently Asked Questions About MDD ICD-10 Codes
What is the most commonly used ICD-10 code for major depressive disorder?
F33.1 (Major Depressive Disorder, Recurrent, Moderate) is one of the most frequently assigned MDD codes in the United States — consistently among the top three most billed codes in outpatient mental health settings. F32.9 (Single Episode, Unspecified) is also extremely common, though it is generally considered a less clinically informative code.
What is the difference between F32 and F33?
F32 codes indicate a patient’s first and only documented episode of major depression. F33 codes indicate recurrent depression — at least two distinct episodes with a period of relative wellness between them. The difference between the two has significant implications for prognosis and treatment planning.
Can a patient have both F32 and F33 codes?
No — a patient receives either F32.x or F33.x, not both. Once a patient has experienced more than one episode, all future coding uses the F33 series regardless of the time elapsed between episodes.
What does F33.1 specifically mean?
F33.1 means the patient has been diagnosed with Major Depressive Disorder, Recurrent, Moderate. This means they have experienced at least two distinct depressive episodes in their lifetime, and the current episode is of moderate severity — significant enough to impair functioning but not severe enough to be completely disabling.
Is F33.1 used for billing insurance?
Yes. F33.1 is a billable ICD-10-CM code used for insurance claims and clinical documentation. It justifies ongoing psychiatric treatment and medication management. Accurate coding is important: if a patient’s chart documents five or more symptoms with clear functional impairment and prior episode history, F33.1 is both clinically and administratively appropriate.
What is the ICD-10 code for treatment-resistant depression?
There is no dedicated ICD-10 code for treatment-resistant depression (TRD) in the current ICD-10-CM system. Treatment-resistant depression is typically documented using the underlying MDD code (e.g., F33.2 for severe recurrent MDD) with clinical notes specifying treatment resistance. This is an area where ICD-10 coding does not yet fully reflect clinical reality.
Does the ICD-10 code change as my condition improves?
Yes. As a patient moves from an active episode into remission, the code is updated to reflect that status — for example, from F33.1 to F33.4 (In Remission, Unspecified) or F33.40/F33.41 depending on whether remission is partial or full. Coding should reflect the patient’s current clinical status, not a fixed historical label.
Can depression be misdiagnosed as a different condition?
Yes — and this matters enormously for both coding and treatment. Bipolar II disorder, in particular, is frequently misidentified as recurrent major depression because the hypomanic episodes are subtle or missed. Treating what is actually bipolar II with antidepressants alone can worsen the overall course. This is one reason accurate diagnosis by an experienced psychiatrist is essential.
Seeking Depression Treatment in Boston
An ICD-10 code is the beginning of a clinical story — not the end of one. What matters most is not the label but whether the diagnosis is accurate, whether the treatment that follows is well-suited to your specific presentation, and whether you have a clinician who is paying close attention as you progress.
At Zen Minds Psychiatry, every patient’s diagnosis is treated as a living assessment — updated as your clinical picture evolves. Whether you’re trying to understand a code on a form, seeking care for the first time, or looking for a second opinion on a diagnosis that hasn’t led to improvement, we’re here to help. Book a consultation with Dr. Amit Chopra at our Boston clinic or via telepsychiatry across Massachusetts.
Zen Minds Psychiatry | Boston, MA | In-person and telepsychiatry | Major Depressive Disorder, Bipolar Disorder, Anxiety, OCD, PTSD, Sleep Disorders | Dr. Amit Chopra, MD — Harvard Medical School Faculty, MGH-affiliated, Mayo Clinic-trained | Call (626) 594-6042 or book online.
Related reading: Major Depressive Disorder Treatment in Boston | Bipolar Disorder Treatment in Boston | CBT vs DBT: Which Therapy Is Right for You? | BPD vs Bipolar Disorder